Carpal tunnel syndrome, or CTS, is a condition in the wrist caused by the compression of the median nerve. This compression can make parts of the hand numb, tingle, or have occasional pain. CTS is a very common problem. More and more cases are from trauma caused by repetitious movements, especially computer use. While CTS can often be successfully treated non-operatively, surgery may be necessary in some cases.
What is the carpal tunnel?
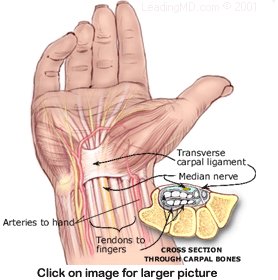
The carpal tunnel is a narrow channel on the palm side of the wrist. Eight bones, called carpals, form an arch creating three rigid walls of the channel. A tight, broad band of tissue, called the transverse carpal ligament, covers the arch and forms a roof over the channel. This "tunnel" is the protective passage for the median nerve and all nine tendons that bend the fingers and thumb. A nerve has two functions:
- to relay information about sensations (like touch, temperature, and pain).
- to control muscles.
The median nerve relays sensations from the thumb, the index finger, the long finger, and the thumb side of the ring finger. This nerve also controls several small muscles in the hand, especially muscles that move the thumb.
What is carpal tunnel syndrome?
Carpal tunnel syndrome, or CTS, is caused by pressure or pinching of the median nerve as it passes through the carpal tunnel on its way to the palm of the hand. For example, there are conditions that can irritate the covering (sheath) of the tendons and can cause this sheath (which also passes through the tunnel) to swell. The tunnel is a rigid, confined space, so any inflammation or swelling in the tunnel can compress the median nerve. This leads to weak and poorly functioning hand muscles. Symptoms may include numbness, tingling, and occasionally pain.
CTS is most often related to work activities that involve repetitive motions, In addition to computer use, the repetitive motions of assembly line workers, cashiers, and hairstylists put them at risk for CTS. Other common causes of CTS are:
- infections or growths within the tunnel that take up space and compress the median nerve.
- osteoarthritis, or other problems with the carpals (wrist bones).
- diseases which cause inflammation or fluid build-up like rheumatoid arthritis, diabetes, and hypothyroidism.
- pregnancy: hormonal changes may cause fluid retention, which can increase pressure on the median nerve. This condition usually improves after pregnancy.
Some people may be born with a condition that puts them at risk to develop CTS. For example, a carpal tunnel that is smaller than average leaves little room for the nerve and tendons. Anything causing swelling around the nerve can increase the pressure on it. The median nerve can only tolerate a small amount of pressure for a short time. Increased pressure over time can cause the hand to "fall asleep". The longer the condition exists, the worse the symptoms become.

 Accredited Business. Rating A+ Click for Review
Accredited Business. Rating A+ Click for Review