Glenohumeral (shoulder) arthritis is a common source of pain and disability that affects up to 20% of the older population. Damage to the cartilage surfaces of the glenohumeral joint (the shoulder's "ball-and-socket" structure) is the primary cause of shoulder arthritis.
There are many treatment options for shoulder arthritis, ranging from pain medications and exercises for mild cases, to surgical procedures for severe cases. Treatment decisions are based upon the cause, the symptoms and the severity of the patient's disease. Each year, over 10,000 shoulder replacement surgeries are performed in the United States to relieve pain and improve function for shoulders that are severely damaged by glenohumeral arthritis.
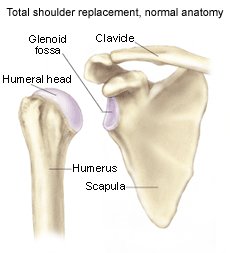
The shoulder is the most mobile joint in the human body with a complex arrangement of structures working together to provide the movement necessary for daily life. Unfortunately, this great mobility comes at the expense of stability. Several bones and a network of soft tissue (ligaments, tendons, and muscles), work together to produce shoulder movement. They interact to keep the joint in place while it moves through extreme ranges of motion. Each of these structures makes an important contribution to shoulder movement and stability. Certain work or sports activities can put great demands upon the shoulder, and injury can occur when the limits of movement are exceeded and/or the individual structures are overloaded.
What is the labrum and what does it do?
The labrum is a disk of cartilage on the glenoid, or "socket" side of the shoulder joint. The labrum helps stabilize the joint and acts as a "bumper" to limit excessive motion of the humerus, the "ball" side of the shoulder joint. More importantly, it holds the humerus securely to the glenoid, almost as if suction were involved. Although the glenoid itself is a relatively flat surface, the labrum's cuff-like contour gives the glenoid a more concave shape. The secure but flexible fit of the humerus within the glenoid permits the great range motion of the healthy shoulder.
Overview
What is glenohumeral joint arthritis?
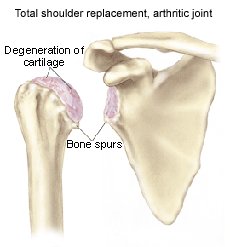
Glenohumeral joint arthritis is caused by the destruction of the cartilage layer covering the bones in the glenohumeral joint. This creates a bone-on-bone environment, which encourages the body to produce osteophytes (bone spurs). Friction between the humerus and the glenoid increases, so the shoulder no longer moves smoothly or comfortably. As osteophytes develop, motion is gradually lost. A number of conditions can lead to the breakdown of cartilage surfaces:
- Wear and tear over time
- Trauma (such as a fracture or dislocation)
- Infection
- A chronic (long-standing) inflammatory condition (such as rheumatoid arthritis)
- Osteonecrosis (bone death caused by loss of blood supply)
- Chronic rotator cuff tears in which the head of the humerus (the upper bone in the arm) loses its proper position in the middle of the glenoid (socket)
- Rare congenital and metabolic conditions
- Post-surgical changes that can be a result of over-tightening during instability surgery
What are the signs and symptoms of glenohumeral arthritis?
Pain from bone-on-bone rubbing within the joint is the most common symptom of glenohumeral arthritis
At first the pain may come and go, but it tends to increase with time, usually over several years.
Movement usually adds to the discomfort.
The pain is commonly present at night, and interferes with sleep.
There may or may not be pain at rest.
Loss of motion is another common symptom. Possible causes of motion loss include:
- Osteophytes that block joint motion
- Constriction of the joint capsule due to chronic inflammation, pain, and disuse
- Fractures or previous surgeries that may have changed joint structure and interfered with motion
- Weakness of the supporting muscles following a rotator cuff tear
Other symptoms may be:
- Atrophy (wasting away) of shoulder muscles due to disuse
- Swelling in the shoulder due to inflammation
- Crepitus (clicking or crunching sound) during shoulder motion
- Tenderness with palpation (touch) affecting the entire shoulder region or specific areas
How is glenohumeral arthritis diagnosed?
The doctor will first obtain a history of the patient's symptoms and health over the past several years. Those who suffer from shoulder arthritis typically report an increase in pain over several years. The doctor will ask if the patient has any conditions that may be the underlying cause of osteoarthritis such as:
- Previous trauma or surgery to the shoulder
- An infection in the shoulder
- A previous rotator cuff tear
- Osteoarthritis or rheumatoid arthritis in other joints
Next, the doctor will do a physical examination of the shoulder to evaluate the symptoms and reveal other conditions that may exist.
X-ray imaging of the shoulder can confirm a diagnosis of glenohumeral arthritis. With x-ray, the doctor can see structural changes that indicate arthritis, such as:
- Irregularity of the joint surface
- Osteophytes, typically located on the lower part of the joint
- Bone erosion on the humeral head, glenoid, or both. Glenoid bone loss is often visible on the backside of the joint.
Other imaging techniques used to make the diagnosis include:
- CT-Scan (Computer Tomography) - This test shows the extent of glenoid bone loss and any anatomic abnormalities that may affect treatment.
- Arthrogram - This technique is useful in the evaluation of rotator cuff tears
- MRI (Magnetic Resonance Image) - Although not as commonly used to diagnose arthritis as other imaging studies, an MRI can provide detailed information about the soft tissue structures of the joint.
How is glenohumeral arthritis treated?
Non-Operative Treatment
Mild glenohumeral arthritis is often manageable with a regimen of:
- Rest
- NSAIDS (non-steroidal anti-inflammatory medicines) - such as ibuprofen or naproxen
- Exercises to increase range of motion and strength
Mild to moderate glenohumeral arthritis pain is often effectively controlled by using any one or a combination of the following treatments:
- Corticosteroid injections (cortisone shots) may be recommended for more severe cases that do not respond to NSAIDS. A concentrated dose of anti-inflammatory medicine is injected directly into the joint and can be safely used to manage most patients' pain. It does not cure the disease, however, and not all patients respond well to the injections. Eventually, corticosteroids lose their effectiveness for most patients' pain.
- Glucosamine and chondroitin are non-prescription supplements that may help neutralize the destructive enzymes associated with osteoarthritis. They may also serve as building blocks for new cartilage formation. These compounds, which are available separately or in combination, have been shown to decrease arthritis pain in some clinical trials; however, more research is needed to evaluate the full extent of their effectiveness.
- Viscosupplementation therapy improves the cushioning of the joint surfaces and has gained popularity in the last few years. Hyaluronic acid is injected directly into the joint in order to improve joint lubrication and reduce friction during movement. Hyaluronic compounds are generally safe although there have been reports of inflammatory reactions in patients treated with some preparations. Most of the studies on viscosupplementation have been done on the knee, so it is less clear what effects this type of treatment will have on the arthritic shoulder.
When severe shoulder arthritis pain is unmanageable with non-operative measures, surgical treatment may be recommended.
Operative Treatment
Debridement
Debridement (removing degenerative tissue and arthroplasty (joint replacement) are the two operative procedures used to treat glenohumeral arthritis. Debridement can be done either with an arthroscope or through a larger incision. Arthroplasty requires an incision.
Debridement:
- Rids the joint of loose cartilage flaps
- Removes enzymes that cause inflammation
- Cleans out loose bodies and osteophytes
- May also include the release of a tight, restrictive joint capsule
In debridement, the physician smoothes the damaged articular cartilage to ease the pain and symptoms associated with the mechanical effects of arthritis (locking, catching, and popping). Debridement may provide temporary pain relief, but does not stop cartilage destruction, which is the primary cause of arthritis pain.
Debridement is usually recommended for patients who are not good candidates for shoulder replacement such as:
- Young people
- Those with a history of joint infection
- Those with loose bodies and small, painful cartilage defects
- Those with mild to moderate joint destruction not severe enough to require shoulder replacement
Both open and arthroscopic debridement techniques have advantages. The arthroscopic procedure has the advantage of being minimally invasive, while open debridement provides greater access to the joint and may permit more complete removal of osteophytes and soft tissue contractures (scar tissue).
Shoulder Arthroplasty (Replacement)
Arthroplasty is the most definitive method to manage the pain associated with severe glenohumeral arthritis. Since 1893, when the first shoulder replacement was performed, shoulder arthroplasty has continued to improve with advances in component materials, instrumentation, and surgical techniques.
Good candidates for shoulder arthroplasty are older patients who will place minimal demands on the shoulder and have no rotator cuff damage.
A total shoulder arthroplasty involves the replacement of both sides of the glenohumeral joint (the humerus and the glenoid). A hemiarthroplasty replaces the humeral head only, and is the treatment of choice when replacement of the glenoid is not advised. The surgeon will recommend a procedure based upon the nature and degree of the patient's arthritis.
Those who should not have shoulder arthroplasty:
- Contact athletes and heavy laborers are not good candidates for shoulder replacement because of the long-term demands they place on the shoulder.
- Total shoulder arthroplasty is not recommended for patients with large, inoperable rotator cuff tears. Since the rotator cuff muscles hold the humeral head tightly to the glenoid, these tears would allow too much movement of the humeral component leading to abnormal loading and loosening of the glenoid component.
- Glenoid replacement is not recommended for patients with isolated humeral head arthritis and normal glenoid cartilage, or those with poor glenoid bone quality.
- Patients with an active infection in the shoulder joint should not have shoulder arthroplasty.
Shoulder arthroplasty is a technically demanding procedure, and the patient should take care to choose an experienced surgeon who has a thorough understanding and knowledge of anatomic and biomechanical principles.
During surgery, the surgeon will:
- Maximize the visual field by appropriately placing incisions and using a good retractor system.
- Maximize the range of joint motion following surgery by removing osteophytes and releasing the joint capsule, if necessary.
- Achieve optimal stability and motion with anatomically correct bone cuts.
- Minimize the chances of post-operative complications with proper recognition and treatment of deficient bone and soft tissue.
- Allow for a quicker rehabilitation and a faster return to activity with a strong repair during closure of the procedure
What types of complications may occur?
Even with the closest attention to detail, surgical complications may occur. Debridement surgery is typically less complex than arthroplasty. However, as with arthroplasty, the potential complications of bleeding, nerve injury, and infection are present.
Some of the more common complications are:
- Infection - Perioperative antibiotics (given before and after surgery) and current intraoperative procedures have reduced infection rates in arthroplasty to less than 1%. If the infection is caught early, aggressive antibiotic treatment may save the components. A chronic infection that has been present for more that 6-12 weeks generally requires removal of the infected implant.
- Blood loss - Although not usually considered a complication, blood loss is common during shoulder replacement surgery and a transfusion may be required. To avoid the concerns of disease transmission from a blood bank, the patient may choose to donate blood for use during the surgery, should it be necessary. Even though there are legitimate concerns about banked blood, the current blood available is extremely safe with very low incidences of disease transmission.
- Nerve injury - Nerve injuries that occur during shoulder replacement surgery are usually temporary, with near normal function returning over time.
- Component failure - This problem is more common with the glenoid component of a total shoulder arthroplasty. Usually, but not always, the loose glenoid component requires surgical removal.
Rehabilitation following shoulder arthroplasty or debridement requires teamwork between the patient, physician, and physical therapist. Good communication will optimize the patient's results and allow the earliest possible return to full activity.
- During the first 6-8 weeks after surgery, the shoulder is usually immobilized with a sling.
- During this time, the therapist will move the shoulder through passive range of motion exercises to prevent stiffness. This will allow the patient to maintain functional motion in the shoulder while protecting the soft tissue repair.
- After the soft tissues are adequately healed (about 6-8 weeks) an active range of motion exercise program can begin.
- Soon after adequate active range of motion is achieved, a strengthening program begins, concentrating on the rotator cuff muscles and those that stabilize the scapula.
- Once appropriate levels of motion and strength are reached, a maintenance program of shoulder exercises, as part of a whole-body fitness regimen, is recommended. The patient who commits to a lifetime physical therapy program will maximize the success of the surgical procedure.
- Return to full activity is highly variable among patients. Generally, complete recovery takes 4-6 months.
How painful is shoulder replacement surgery?
Shoulder arthroplasty is a complex procedure, which requires a great amount of cutting of deep tissues and bone. The surgeon takes great care to eliminate pain with appropriate analgesia both immediately after surgery and during the rehabilitation process. A long acting local anesthetic infused around the nerves of the joint is often used with general anesthesia during surgery. These regional blocks will provide several hours of pain relief even after a patient has emerged from general anesthesia. A patient-controlled intravenous infusion pump (PCA) is used in the early post-operative period for pain control. By the second or third day after surgery, oral pain relief medication is adequate through the early rehabilitation period (4-6 weeks).
How long before I can return to my normal activities after shoulder arthroplasty?
The time it takes to return to normal activity varies greatly from patient to patient. Most individuals have less pain at night or at rest in the first 2-4 weeks after surgery. Pain with activity persists longer, but generally decreases as the strength and function of the shoulder muscles improve. Full recovery usually takes 4-6 months.
What activities can I safely do after shoulder replacement?
The goal of shoulder arthroplasty is to relieve the pain from glenohumeral arthritis. It is unrealistic to expect to return to repetitive, heavy, overhead activities, which would put the replacement components at risk. Shoulder function after arthroplasty is also unlikely to allow the motions required by these activities.
According to the American Shoulder and Elbow Society, the acceptable activities after a shoulder arthroplasty are:
- bowling, doubles tennis, cross-country skiing, swimming, canoeing, and shuffleboard
- for those with previous experience in the activity: golf, ice skating, shooting, and downhill skiing
Unacceptable activities are:
- football, gymnastics, hockey, rock climbing
- throwing sports, except for gentle underhand tossing
I've heard that joint replacements sometimes "wear out" and need to be redone. What are the chances I may require a second shoulder arthroplasty?
Long-term studies show that 85-90% of total shoulder replacements are functioning well ten years after implantation, and 75-85% are doing well fifteen years after surgery. Over time, current advances in materials and techniques should improve these percentages even more.
Gartsmann GM, Roddey TS, Hammerman SM. Shoulder arthroplasty with or without resurfacing of the glenoid in patients who have osteoarthritis. Journal of Bone and Joint Surgery. 82-A: pp 26-34, 2000.
Sperling JW, Cofield RH, Rowland CM. Neer hemiarthroplasty and Neer total shoulder arthroplasty in patients fifty years old or less: Long-term results Journal of Bone and Joint Surgery. 80-A: pp 464-73, 1998.
Lynch NM, Cofield RH, Silbert PL, Hermann RC. Neurologic complications after total shoulder arthroplasty. Journal of Shoulder and Elbow Surgery. Vol 5: pp53-61, 1996.


 Accredited Business. Rating A+ Click for Review
Accredited Business. Rating A+ Click for Review